What 5,000 Behavioral Health Websites Reveal About Patient Accessibility.
An analysis of nearly 5,000 behavioral health provider websites shows consistent gaps in insurance, admission, and empathetic content across the industry.
- Introduction
- Methodology
- Finding #1: What Providers Actually Talk About
- Finding #2: Where’s the Warmth?
- Finding #3: Will My Insurance Cover This?
- Finding #4: The Differentiation Problem
- Finding #5: Faceless Providers
- Finding #6: The Admission Bottleneck
- Finding #7: Conversion Readiness
- Finding #8: Internal Link Strategy
- The Intent Pyramid
- Practical Implications
- Conclusion
Introduction
The decision to seek behavioral health treatment comes after difficult conversations, mounting consequences, or a moment of clarity. When that person finally searches for help, what do they find on most provider websites?
Research shows that 77% of healthcare journeys begin with an online search. For behavioral health specifically, where stigma, uncertainty, and crisis often intersect, that first digital touchpoint may be the only chance a provider has before a potential patient gives up or reaches out to a competitor.
To answer this question, I conducted a comprehensive analysis of 4,957 behavioral health provider websites, examining 85,421 individual pages and mapping 882,286 internal links. I classified content by intent, measured empathy using a peer-reviewed NLP framework, and assessed conversion readiness across the industry.
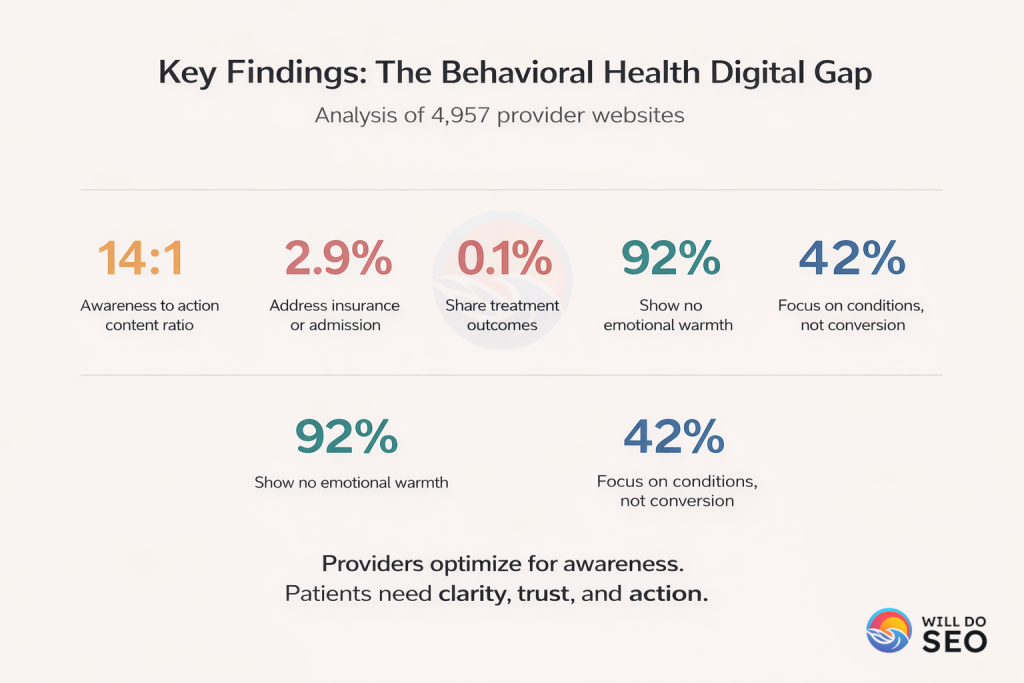
The findings show a consistent pattern: providers have optimized their digital presence for awareness, telling patients “here’s what we do,” while leaving them without answers, without warmth, and without clear next steps at the moment they’re ready to act.
The gaps aren’t in general content. They’re in the specific information that helps patients take action.
Methodology
This analysis draws from the SAMHSA (Substance Abuse and Mental Health Services Administration) treatment locator database, the most comprehensive source of U.S. behavioral health facilities. From the initial database of 27,149 facility records, I extracted 8,141 unique website domains, then focused the analysis on private providers (excluding .gov and .edu domains).
After geographic stratification across all 50 states and website validation, the final sample includes 4,957 private behavioral health provider websites, representing approximately 63.1% of private providers with an active web presence.
What I Measured
For each website, I crawled up to 100 pages, capturing content, internal links, and page structure. The analysis included:
Intent Classification
Using zero-shot classification with a state-of-the-art natural language inference model (DeBERTa-v3-large, trained on MNLI, FEVER, ANLI, and WANLI datasets with 435 million parameters), I categorized pages across 14 intent types. Unlike keyword-based approaches that detect mentions, this method determines what each page is primarily about through semantic understanding by testing natural language hypotheses against page content. For each page, I extracted: title, H1, meta description, and first 800 characters of body content, then classified against descriptive labels for each intent category. The model returns confidence scores for all 14 categories; the highest-scoring category becomes the primary intent.
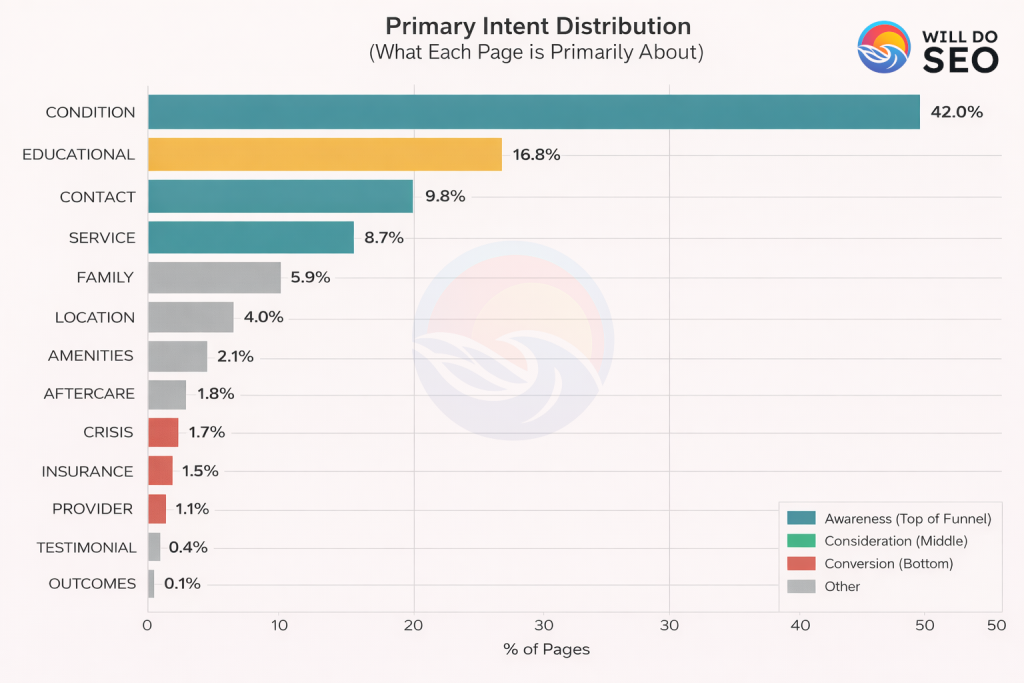
Categories: CONDITION, EDUCATIONAL, SERVICE, CONTACT, FAMILY, LOCATION, AMENITIES, AFTERCARE, CRISIS, INSURANCE, ADMISSION, PROVIDER, TESTIMONIAL, OUTCOMES.
Empathy Analysis
Using the Sharma et al. (2020) EPITOME framework published in “A Computational Approach to Understanding Empathy Expressed in Text-Based Mental Health Support” (EMNLP 2020), I measured three dimensions of empathy in text:
- Emotional Reactions (ER): Expressions of warmth, compassion, and concern
- Interpretations (IP): Communicating understanding of feelings and experiences
- Explorations (EX): Probing questions to improve understanding
I trained their RoBERTa-based bi-encoder models on their human-annotated Reddit mental health dataset (10,000+ labeled conversations), then ran inference on all 85,421 crawled pages. Each page received scores for all three dimensions, which were aggregated into domain-level empathy scores.
GitHub: https://github.com/behavioral-data/Empathy-Mental-Health
Conversion Elements
I scanned page content for specific conversion-enabling patterns using keyword detection:
- Appointment Booking: “schedule”, “book”, “appointment”
- Phone CTAs: “call now”, “call us”, “phone”, “1-800”, “1-888”
- Contact Forms: “contact form”, “fill out”, “submit”
- Chat Widgets: “chat”, “live chat”, “chat now”
- Insurance Verification: “verify insurance”, “check coverage”, “insurance verification”
Each page was flagged for the presence of each element, then aggregated to determine which providers have conversion infrastructure in place.
Differentiation Analysis
I identified providers making uniqueness claims by scanning content for differentiation language:
- Vague Claims: “unique”, “different”, “unlike other”, “one-of-a-kind”, “special approach”, “not like other facilities”
- Substantive Evidence: Presence of specific differentiators (proprietary programs, unique methodologies, specific outcome data, named frameworks, accreditations with context)
Pages were categorized as: (1) making vague claims with no substance, (2) making claims with supporting evidence, or (3) no differentiation claims. This reveals the gap between providers claiming uniqueness versus demonstrating it.
Staff Visibility
I assessed provider transparency by analyzing staff-related content:
- Staff Pages: URL patterns containing “team”, “staff”, “providers”, “therapists”, “about-us”, “our-team”
- Credentials: Keywords like “licensed”, “certified”, “credentials”, “LPC”, “LCSW”, “PhD”, “MD”
- Photos: Presence of staff imagery indicators
- Bios: Detailed biographical content with specialties and backgrounds
Providers were scored on a 0-5 scale based on how many of these elements were present, revealing how transparent providers are about who will provide care.
Internal Link Analysis
Using NetworkX graph analysis, I constructed a directed graph of all internal links (882,286 edges across 305,566 nodes) and calculated:
- PageRank: Google’s link-based authority metric (damping factor 0.85)
- In-Degree/Out-Degree: Number of pages linking to/from each page
- HITS Algorithm: Hub scores (pages that link to authorities) and Authority scores (pages linked by hubs)
- Betweenness Centrality: Pages that serve as critical bridges between site sections
- Click Depth: Minimum clicks required to reach each page from homepage (BFS traversal)
Link Position Classification: For each link, I identified its HTML location using CSS selectors:
- Header/Main Navigation
- Footer Navigation
- Sidebar Navigation
- Breadcrumb Navigation
- Content Body Links
- CTA Buttons
- Mega Menu/Dropdowns
- Related Posts Sections
This reveals not just what providers link to, but how prominently they feature those links in their site architecture.
Time Investment
This analysis required approximately 130-144 hours of compute and development time:
- Data Acquisition: 72 hours crawling 85,421 pages across 4,957 domains
- Intent Classification: 21 hours running zero-shot inference with DeBERTa-v3-large
- Empathy Model Training: 4 hours training three RoBERTa bi-encoder models
- Empathy Inference: 3 hours scoring 85,421 pages across three empathy dimensions
- Link Graph Analysis: 9 hours constructing and analyzing a graph of 305,566 nodes and 882,286 edges
- Development & Analysis: 35 hours for pipeline development, QA, and visualization
By the Numbers
The dataset encompasses:
- Approximately 79 million words of content
- 4,957 provider websites
- 85,421 pages analyzed
- 882,286 internal links mapped
Statistical Significance
A natural question when reviewing these findings is how confident can we be that these patterns reflect the broader industry, not just the sample?
The population of private behavioral health providers with validated websites totals 7,854 domains. The sample of 4,957 providers represents 63.1% coverage of this population, an unusually high proportion for industry research of this type.
Using standard margin of error calculations with a 95% confidence level and finite population correction, the margin of error is approximately ±0.8 percentage points.
In practical terms, this means:
- When I report that 89.7% of providers lack insurance content, the true population value falls between 88.8% and 90.4% with 95% confidence
- When I report that 92% of pages show no emotional warmth, the true value falls between 91.2% and 92.8%
- The findings are statistically robust for drawing industry-wide conclusions
The high sample coverage and low margin of error mean these aren’t tentative observations. They represent reliable patterns across the private behavioral health provider market.
Finding #1: What Providers Actually Talk About
Using zero-shot classification with a state-of-the-art natural language inference model (DeBERTa-v3-large), I analyzed what each of the 85,421 pages is primarily about. This goes beyond keyword detection to understand semantic meaning.
The distribution unearths where providers invest their content resources:
Finding #2: Where’s the Warmth?
Perhaps the most interesting finding involves empathy, or rather, its absence.
Using the peer-reviewed Sharma et al. (2020) EMNLP framework for measuring empathy in mental health text, I analyzed how provider websites actually communicate with potential patients. This framework measures three dimensions:
- Emotional Reactions: Expressions of warmth, compassion, and care
- Interpretations: Demonstrating understanding of feelings
- Explorations: Probing and showing genuine engagement
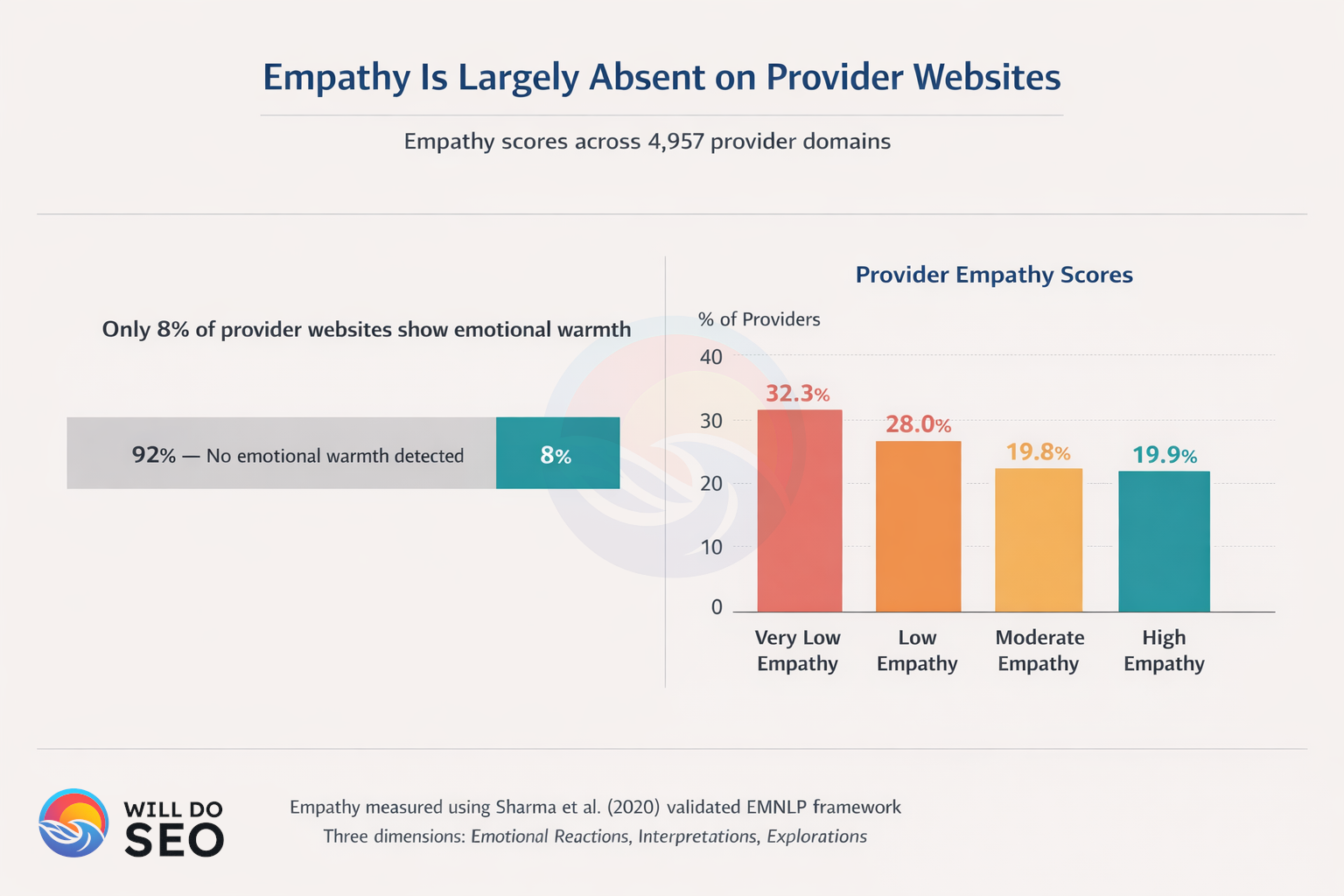
92% of pages show no emotional warmth whatsoever.
Looking at provider-level scores, 32.3% of domains have very low empathy scores (below 0.1 on a 0-1 scale). The mean empathy score across all providers is just 0.138, with a median of 0.090.
Why This Matters
Patients seeking behavioral health support are often in vulnerable states. The decision to search for treatment, whether for addiction, depression, anxiety, or other conditions, frequently comes during moments of crisis or after significant internal struggle.
The first digital touchpoint sets expectations for the care experience. When that touchpoint reads like clinical documentation rather than a compassionate welcome, it creates a disconnect. Clinical, neutral language, while professional, can feel cold and impersonal to someone who has finally worked up the courage to seek help.
There’s an irony here: providers talk about empathy in their mission statements. “We provide compassionate care.”, “Our caring team is here for you.” But the actual content of their websites, the pages where patients land, the descriptions they read, often lacks that same compassion in practice.
Healthcare content shouldn’t read like a textbook when someone is in crisis.
Finding #3: Will My Insurance Cover This?
“Does my insurance cover rehab?” is one of the most common search queries related to behavioral health treatment. Cost and coverage represent the number one barrier to treatment for many patients. At the moment someone decides they need help, this is often their most pressing practical question.
Yet the analysis found:
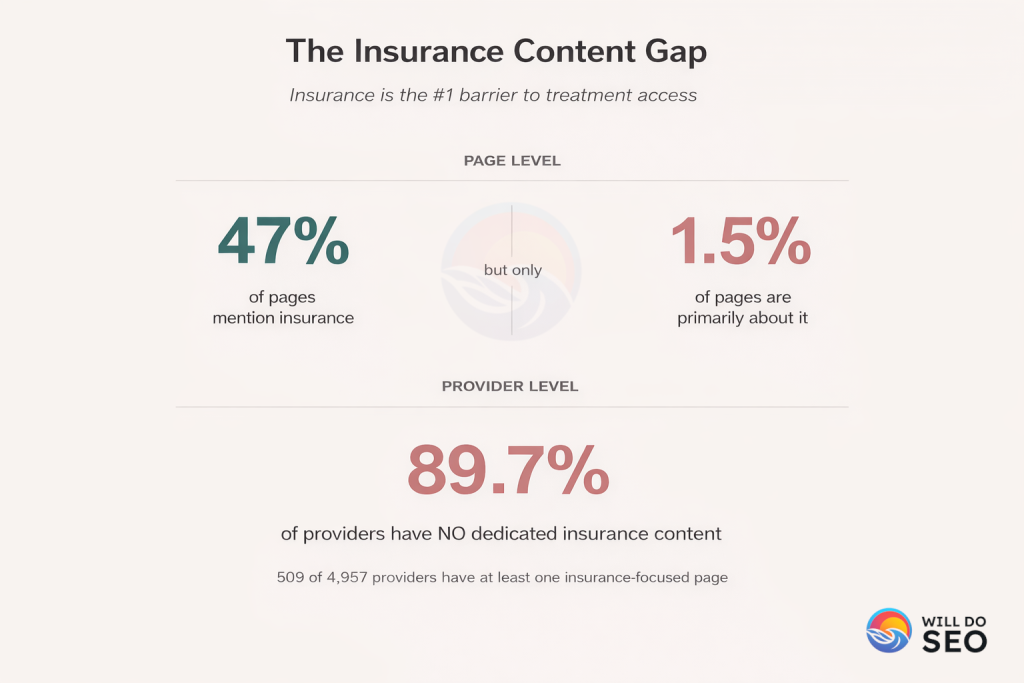
- 47% of pages mention insurance at all
- Only 1.5% of pages are primarily about insurance (1,295 pages total)
- That’s an average of just 0.26 insurance pages per provider
- Only 3.8% of sites have insurance verification tools
- 89.7% of providers have no meaningful insurance content whatsoever
The disconnect is profound. Providers know patients ask about insurance. Anyone who has taken an intake call knows this is often the first question. Yet 89.7% of providers make patients call to find out whether treatment is even financially accessible.
In a crisis moment, that friction can mean losing the patient entirely. Someone searching at 3 AM, trying to understand their options, encounters a wall: “Call us to learn more.” The motivation that drove them to search may not last until business hours.
What Patients Need to See
Effective insurance content doesn’t require a complex verification system. At minimum, patients want to know:
- What insurance plans are accepted
- How verification works
- What options exist if they don’t have insurance
- Approximate out-of-pocket costs when possible
Even basic text addressing these questions would differentiate a provider from 89.7% of competitors.
Finding #4: The Differentiation Problem
In a crowded market, providers naturally want to stand out. But claiming to be different and actually demonstrating that difference are two separate things.
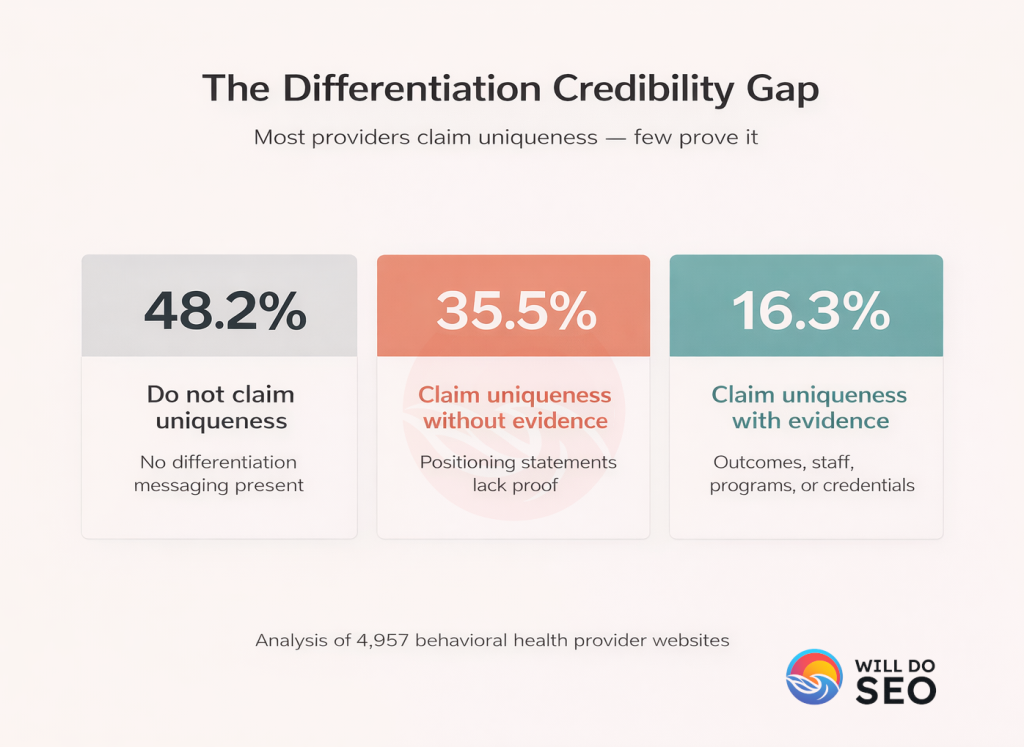
The analysis found:
- 51.8% of providers (2,567 of 4,957) claim to be “unique,” “different,” or use similar differentiating language
- Of those who claim differentiation, 68.5% back it up with some form of evidence
- 31.5% (808 providers) provide no evidence to support their uniqueness claims
The most common empty phrases include “unique approach,” “different from other facilities,” “what sets us apart,” and “stands out from the crowd,” all without substantive follow-through.
What Counts as Evidence?
Providers who successfully differentiate themselves typically include:
- Specific accreditations (Joint Commission, CARF)
- Outcome data and success metrics
- Proprietary or specialized methodologies
- Focus on specific populations or conditions
- Named evidence-based practices
- Staff credentials and specializations
Without these specifics, differentiation claims become noise. Patients have heard “we’re unique” from every provider they’ve researched. When 31.5% of providers who claim uniqueness can’t articulate why, the claim becomes meaningless, or worse, it signals that the provider may not actually know what makes them different.
Finding #5: Faceless Providers
Trust is foundational to behavioral health treatment. Patients are being asked to share their deepest struggles, their fears, their trauma. Before doing so, they naturally want to know who will be treating them.
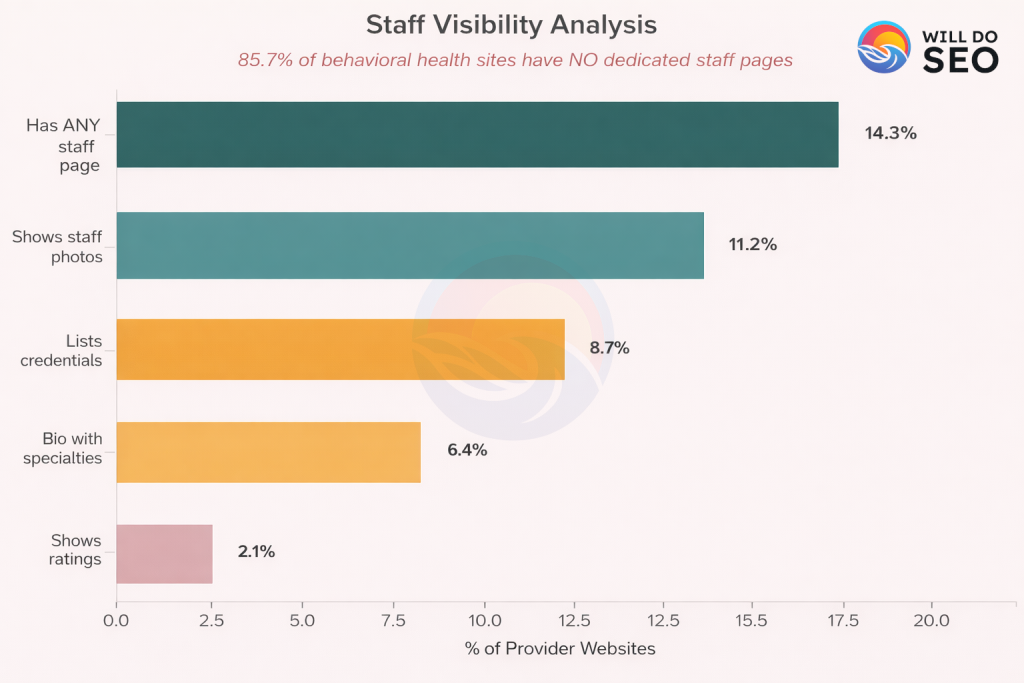
- 85.7% of providers have no dedicated staff or team pages
- Only 14.3% showcase their clinical team
- While 88% mention staff on their homepage, it’s usually generic (“our experienced team”) with no substance
- 12% don’t mention staff anywhere on their homepage
Credential Visibility
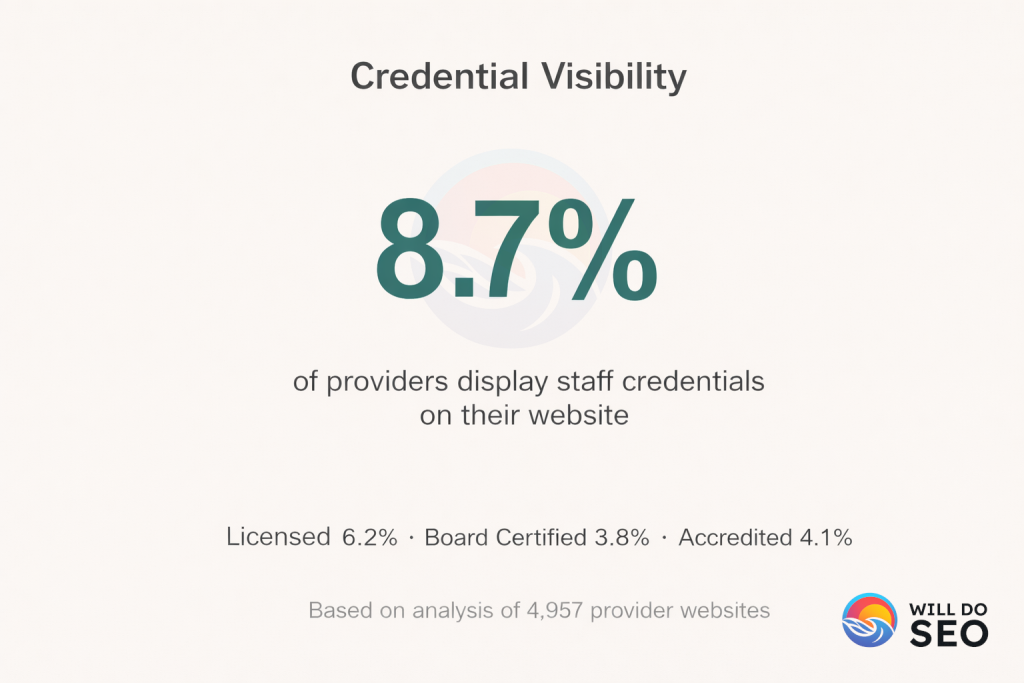
Among providers who do display credentials:
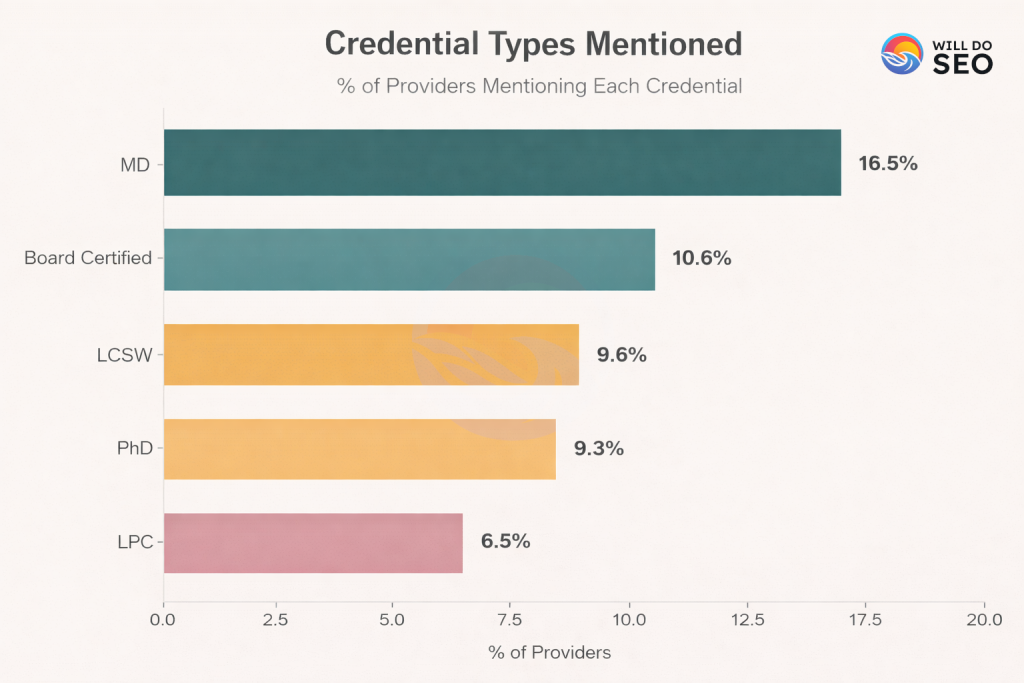
Consider the contrast with other healthcare sectors. Patients routinely research doctors before medical procedures, reviewing credentials, experience, and patient reviews. Yet in behavioral health, where the therapeutic relationship may be even more critical to outcomes, the vast majority of providers offer no visibility into who provides care.
Mentioning “our experienced team” is not the same as showing the team. Staff pages humanize providers, build trust, and give patients confidence that they’ll be treated by qualified professionals.
Finding #6: The Admission Bottleneck
A patient has done their research. They’ve decided they need help. They’ve overcome the stigma, the fear, the uncertainty. Now they have one question: “What happens next?”
The analysis found that most providers leave this question unanswered:
- Only 11.2% of pages mention the admission process
- Just 1.4% of pages are primarily about how to get started
- Only about 1 in 4 providers have a dedicated page explaining how to get started
What Patients Want to Know
The decision to seek treatment is just the beginning. Patients are often facing the unknown, and uncertainty creates friction. They want answers to practical questions:
- What happens when I call?
- What should I bring?
- How long does intake take?
- What can I expect on day one?
- Who will I be speaking with to learn more?
- What’s the timeline from first call to starting treatment?
The gap between “I want help” and “I’m getting help” is where patients may fall through. Every unanswered question is a potential drop off point. Providers who shine light on the admission process reduce anxiety and increase the likelihood that someone who’s ready to act actually follows through.
Finding #7: Conversion Readiness
When someone is ready to take action, is the website ready to help them?
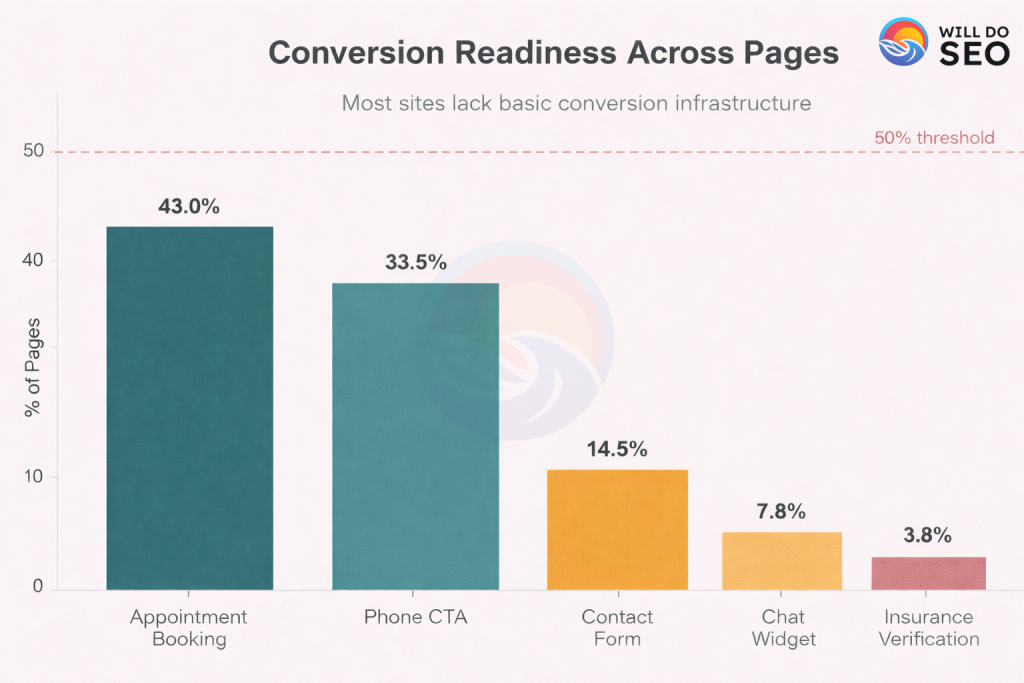
I analyzed pages for the presence of conversion elements:
| Conversion Element | % of Pages |
|---|---|
| Appointment booking | 43.0% |
| Phone CTA | 33.5% |
| Contact form | 14.5% |
| Chat widget | 7.8% |
| Insurance verification | 3.8% |
37.3% of pages have no conversion elements at all. Over a third of all content pages are dead ends, informational cul-de-sacs with no clear path to action.
Finding #8: Internal Link Strategy
Internal linking, how pages connect to each other, reveals strategic priorities and affects both user experience and search visibility.
Across the dataset, I mapped 882,286 internal links. The distribution reveals where providers place navigational emphasis:
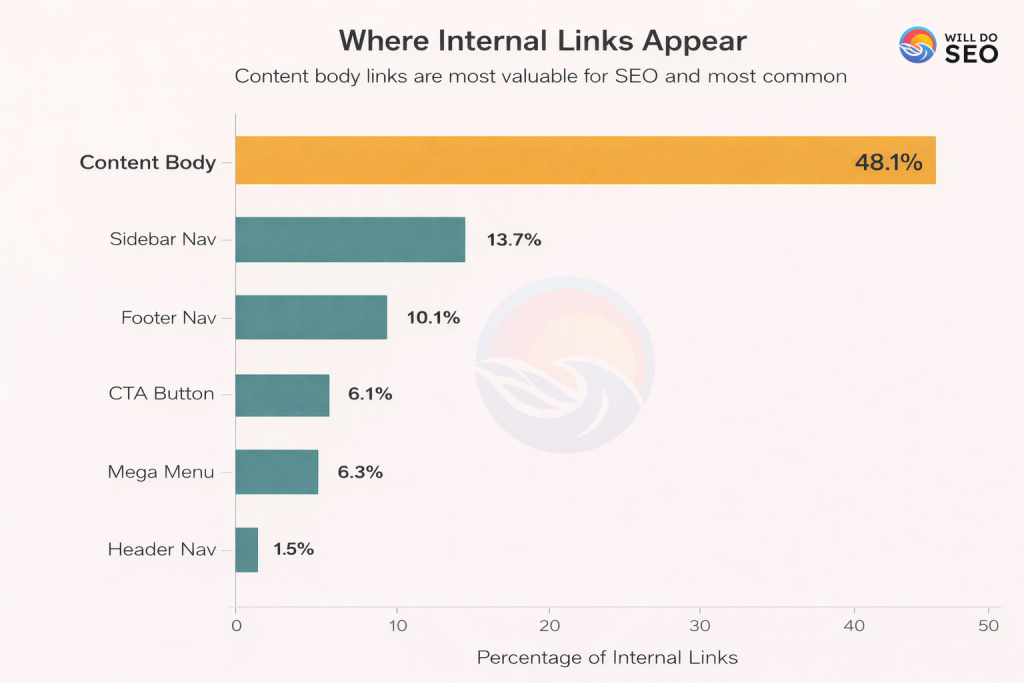
Several patterns emerge:
Contextual links dominate: 37% of links appear within content, which is good for SEO. In-content links provide relevant pathways when users are engaged with a topic.
CTA links are underutilized: Only 7.8% of links are action focused CTA buttons. Driving conversions is the ultimate goal, this represents a missed opportunity.
Significant difference exists: The mean number of links per provider is 196, while the median is just 13, a 15x gap indicating huge variation between well-structured sites and those with minimal internal linking.
Empty link anchor text is common: 9.2% of links have no anchor text, providing no context for users or search engines about where the link leads.
The Intent Pyramid
When I mapped content distribution against patient journey stages, a clear inversion emerged:
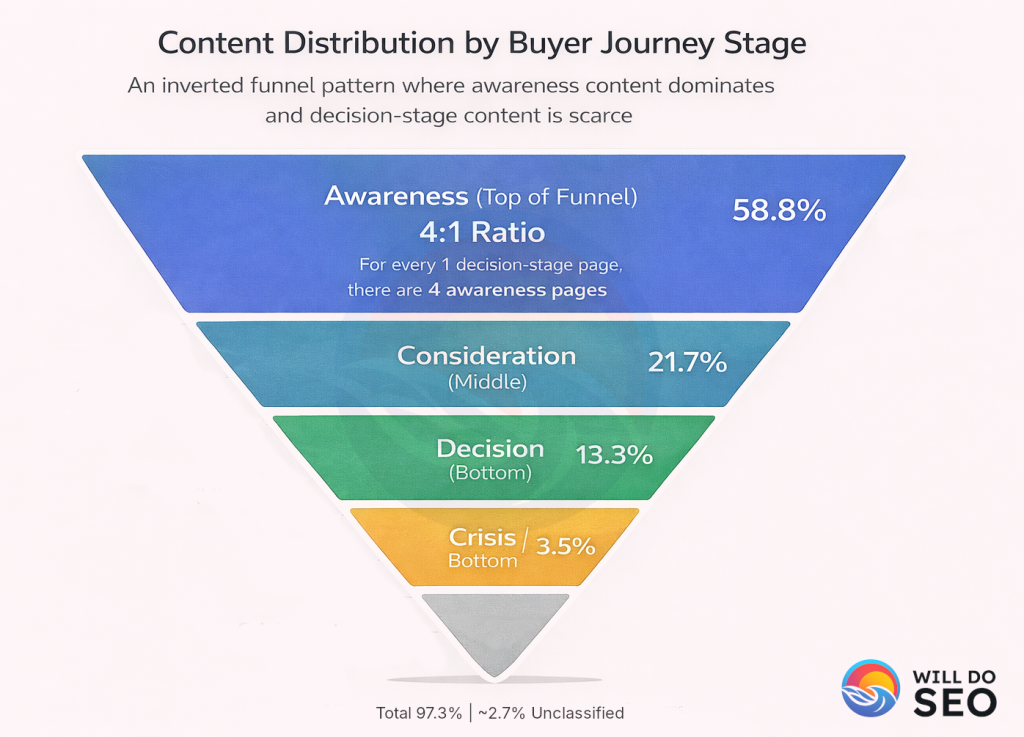
- AWARENESS (Exploring): Services and educational content dominate. This is where providers invest the most, explaining what conditions are, what treatments exist, and what services they offer.
- EVALUATION (Comparing Options): Provider information, location details, and condition-specific content help patients assess and compare options.
- ACTION (Ready to Decide): Insurance and admission content, the information patients need when ready to act, represents the smallest share of all content.
The funnel is inverted from patient needs. Providers invest heavily in awareness content, moderately in evaluation content, and minimally in action content. Yet patients ready to convert, those who have already decided they need help, find the least support precisely when it matters most.
Practical Implications
These findings point to specific, and actionable improvements that any provider can implement. These gaps are so consistent across the industry, addressing them can create an immediate differentiation.
1. Add Insurance Content Immediately
With 89.7% of providers missing insurance content entirely, this represents the single biggest quick win. At minimum, create a dedicated page answering:
- What insurance plans do you accept?
- How does the verification process work?
- What options exist for uninsured patients?
- Are payment plans available?
If possible, add an insurance verification widget. Only 3.8% of sites currently have one.
2. Create an Admission Journey Page
Demystify the unknown. Walk patients through exactly what happens from first contact through the beginning of treatment:
- What to expect when they call
- The intake and assessment process
- Timeline from first contact to treatment start
- What to bring on day one
- Who they’ll meet and when
One comprehensive page addressing these questions can change conversion rates, and ~85% of competitors don’t have this content.
3. Write With Empathy, Not Just About Empathy
Review your website content with fresh eyes. Does it read like clinical documentation or a compassionate welcome? Consider:
- Using language that acknowledges the patient’s struggle
- Leading with understanding rather than credentials
- Replacing “Our services include…” with “We understand how hard this decision is…”
- Balancing professionalism with warmth
Tone is free to change. 92% of competitor content lacks emotional warmth. Writing with genuine compassion differentiates immediately.
4. Show Your Staff
Create dedicated staff pages with:
- Photos (with permission)
- Credentials and certifications
- Brief bios including specialties
- Personal treatment philosophies when appropriate
85.7% of competitors have no staff pages. Patients want to know who will treat them. Providing this builds trust before the first conversation.
5. Back Up Differentiation Claims
If your website claims you’re unique, audit those claims:
- Is the claim followed by specific evidence?
- Can you name accreditations, methodologies, or outcomes?
- Do you specify what populations or conditions you specialize in?
If a differentiation claim isn’t backed by substance, either add the evidence or remove the claim. Generic uniqueness claims without support may damage credibility.
6. Enable Immediate Response
Consider the 3 AM searcher:
- Add a chat widget for crisis moments (even if staffed only during certain hours, it signals availability)
- Ensure phone CTAs are visible above the fold
- Make after-hours options clear
- If chat isn’t feasible, at least provide clear expectations about response times
Only 7.8% of pages currently offer immediate response capability. This is a significant gap.
The Competitive Reality
These aren’t difficult fixes. They don’t require massive budgets or complete website redesigns. Yet because the gaps are so consistent across the industry, addressing even a few of these issues creates meaningful differentiation:
- 89.7% don’t have insurance content. Adding it is instant differentiation, and great for search visibility, especially with a local / GEO focus.
- ~85% lack admission guidance. One page could change conversion.
- 92% lack empathetic language. Tone is free to change.
- 85.7% have no staff visibility. A few bios build trust.
Conclusion
Across 4,957 behavioral health provider websites, representing approximately 63.1% of the private provider market, the analysis reveals consistent gaps in patient accessibility:
- 92% of pages lack emotional warmth (validated empathy analysis)
- 89.7% of providers have no insurance content
- 85.7% have no dedicated staff pages
- ~85% lack admission process guidance
- 37.3% of pages have no conversion elements
- 31.5% of providers claiming “uniqueness” provide no evidence (808 providers)
- Only 7.8% offer immediate response capability (chat)
Providers have optimized for awareness, telling patients “here’s what we do,” while leaving them without answers, without warmth, and without clear next steps at the moment they’re ready to act.
For patients searching during a crisis, this creates friction where there should be pathways. Someone who has finally decided to seek help finds detailed descriptions of treatment modalities but no clear answer to whether their insurance is accepted. They find claims of compassionate care in clinical language. They find “call us” where there should be “here’s how to start.”
The gaps are consistent across the industry, which means addressing them provides significant differentiation. The content patients need most is the content providers create least. That’s both the problem and the opportunity.
I’ll be digging deeper into treatment coverage, population focus, content depth, and how all of this ties into search visibility in the coming weeks.
Limitations
As with any analysis of this scope, important limitations apply:
Crawl depth was capped: I limited crawls to 100 pages per provider. Larger sites were sampled rather than exhaustively crawled, which means some content may not be captured in the analysis.
Point-in-time snapshot: Data was collected in December 2025. Websites change, and individual provider results may have shifted since collection.
Private providers focus: Hospital systems and government-run facilities are not represented. Results reflect the private behavioral health provider market.
Conversion outcomes unknown: I can measure conversion element presence but cannot measure actual patient conversion. Presence of a chat widget doesn’t guarantee effectiveness.
Content quality not assessed: Presence of content is not the same as quality. A page mentioning insurance may still be inadequate or confusing.
Citations & References
Empathy Analysis Framework
Sharma, A., Miner, A.S., Atkins, D.C., & Althoff, T. (2020). A Computational Approach to Understanding Empathy Expressed in Text-Based Mental Health Support. Proceedings of the 2020 Conference on Empirical Methods in Natural Language Processing (EMNLP), 5263-5276. Association for Computational Linguistics.
Paper: https://aclanthology.org/2020.emnlp-main.425/
Code: https://github.com/behavioral-data/Empathy-Mental-Health
Intent Classification Model
Laurer, M., van Atteveldt, W., Casas, A., & Welbers, K. (2024). Less Annotating, More Classifying: Addressing the Data Scarcity Issue of Supervised Machine Learning with Deep Transfer Learning and BERT-NLI. Political Analysis, 32(1), 84-100.
Model: MoritzLaurer/DeBERTa-v3-large-mnli-fever-anli-ling-wanli
HuggingFace: https://huggingface.co/MoritzLaurer/DeBERTa-v3-large-mnli-fever-anli-ling-wanli
DeBERTa Architecture
He, P., Liu, X., Gao, J., & Chen, W. (2021). DeBERTa: Decoding-enhanced BERT with Disentangled Attention. International Conference on Learning Representations (ICLR 2021).
Paper: https://arxiv.org/abs/2006.03654
Graph Analysis
Hagberg, A.A., Schult, D.A., & Swart, P.J. (2008). Exploring Network Structure, Dynamics, and Function using NetworkX. Proceedings of the 7th Python in Science Conference (SciPy 2008), 11-15.
Documentation: https://networkx.org/
GitHub: https://github.com/networkx/networkx
PageRank Algorithm
Page, L., Brin, S., Motwani, R., & Winograd, T. (1999). The PageRank Citation Ranking: Bringing Order to the Web. Stanford InfoLab Technical Report.
Paper: http://ilpubs.stanford.edu:8090/422/
HITS Algorithm
Kleinberg, J.M. (1999). Authoritative Sources in a Hyperlinked Environment. Journal of the ACM, 46(5), 604-632.
Paper: https://doi.org/10.1145/324133.324140
Web Crawling
Firecrawl API – Web scraping and crawling service.
Documentation: https://docs.firecrawl.dev/
Machine Learning Framework
Wolf, T., et al. (2020). Transformers: State-of-the-Art Natural Language Processing. Proceedings of the 2020 Conference on Empirical Methods in Natural Language Processing: System Demonstrations, 38-45.
HuggingFace Transformers: https://huggingface.co/transformers/
GitHub: https://github.com/huggingface/transformers
Data Source
SAMHSA (Substance Abuse and Mental Health Services Administration). FindTreatment.gov Facility Locator.
Website: https://findtreatment.gov/
WillDoSEO.com
Design Support from maybeitsdavemeline.com 🎨
Powered By Espresso ☕️
